My elective amputation was a last-ditch effort to allow me the best hand function with the least amount of pain. And it was the result of a rare and terrible condition called Interosseous-Lumbrical Adhesions, or Saddle Syndrome. There is very little information on this condition so I am hoping that by sharing my experience, it will help add to the knowledge and maybe prevent someone else from having to go on the long journey I did in order to find relief.
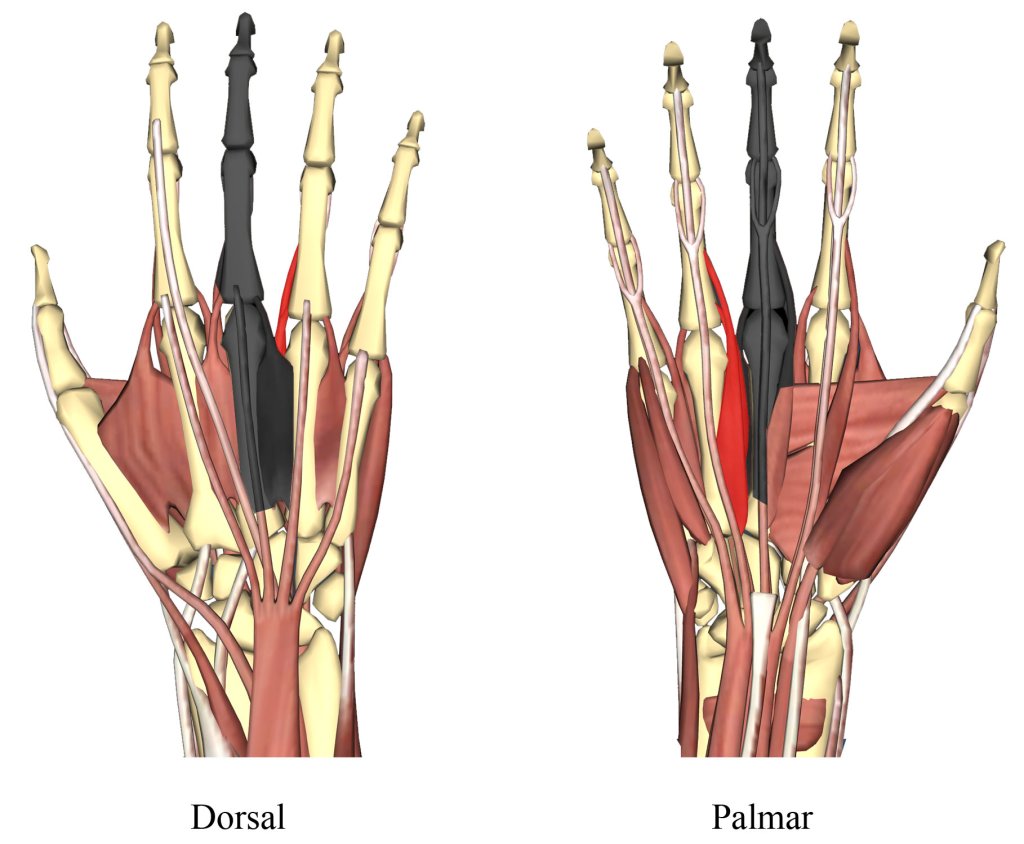
Saddle Syndrome is a painful condition resulting from scar tissue in the palm of the hand. The palm is full of small muscles as well as tendons and ligaments that work in intricate coordination to move our fingers. With Saddle Syndrome, scar tissue adheres to some of the muscles and crosses the deep transverse metacarpal ligament (dTML) that holds the knuckles in place. The name comes from the scar tissue sitting across the dTML like a rider atop a horse. Besides making finger movements more difficult, the scar tissue impinges on the ligament and is very painful. Imagine a piano where someone has poured tar across the keys. You might still be able to play music, but it would be difficult. In my case, scar tissue also pulled on a tendon, causing it to slap on a nerve and result in blinding pain.
Saddle Syndrome doesn’t show up on x-rays or MRIs, it is a diagnosis of exclusion until it can be confirmed via surgery.* But performing surgery on the hand can create more scar tissue, so surgeons aren’t usually eager to slice one open unless they have good cause. In my case, every surgeon who has worked on my hand has commented on the copious amounts of scar tissue they found, the last surgeon spent an extra hour just cleaning out scar tissue! Because it is painful and a diagnosis of exclusion, Saddle Syndrome is considered a “controversial musculoskeletal pain condition”1 and not all surgeons think it is a genuine condition. I went through many surgeons and incorrect diagnoses before I figured out I had Saddle Syndrome, and even then I had to find a surgeon who would believe me. A study in 2015 observed that it primarily occurred in females who had made workman’s comp claims and that the “biopsychosocial aspects of patients with saddle syndrome need to be further studied to determine the underlying factors involved in the etiology.”1 In other words, because Saddle Syndrome can’t be easily diagnosed and it has occurred to women who got injured on the job, how can a surgeon be sure that is isn’t just a woman trying to get money by claiming they have pain? Surely hand size and/or a predisposition to scar tissue formation couldn’t possibly be factors?
According to one study, only 0.4% of patients seen across clinics have Saddle Syndrome, making it extremely rare.2,3 After my first surgery, the surgeon called me a textbook case, the first patient with the condition that they had seen in five years. It is usually the result of a crush injury, although other causes, such as infection3, have also been observed. In my case, it was a the result of a high energy torsion injury, a rare case among rare cases. (I calculated nearly 900lbs of force went into my hand at the time of injury.) I had the classic scar tissue formation across the dTML, and the first surgery tried to minimize the scar tissue and impingement on the ligament as much as possible by removing both scar tissue and some of the ligament. But I had even more extensive scar tissue in the third dorsal interosseous, the V-shaped muscle between the middle and ring fingers on the back of the palm, that the surgeon never saw. I found another surgeon who worked with me to find innovative approaches to eliminating the pain while keeping as much function of my middle finger as possible, but in the end we both agreed that removing the finger and the badly damaged muscle was the best solution for my case. When my surgeon saw how much the amputation changed my whole personality, he apologized for not doing it sooner.
I had to fight for nearly four years to escape a life of chronic pain. I went to countless surgeons, had hours upon hours of physical therapy, and had as many incorrect diagnoses as I had shoulder shrugs from medical professionals. I hope that if you have Saddle Syndrome, you are able to find a solution much faster than I did! And if you are a medical professional, I hope my story will make you think twice before dismissing a patient’s traumatic hand pain as psychosomatic.
*Because of the industry I was working in at the time, I was able to have someone with an ultrasound machine take a look at the damaged part of my hand, and although they were unable to diagnose what they saw, the results were clearly abnormal. Perhaps ultrasound could be used in the future to help diagnose Saddle Syndrome.
1 Shah, S., Bachoura, A., Jacoby, S.M., George, B., Culp, R.W. (2015) Pyschosocial Factors in Patients diagnosed with Saddle Syndrome of the Hand. AAHS Annual Meeting. Retrieved from https://meeting.handsurgery.org/abstracts/2013/28.cgi
2 Dancea, H.C., Manuskakian, H., Thirklannad, S.T. (2015) Saddle Syndrome – a Non-Operative Approach. AAHS Annual Meeting. Retrieved from https://meeting.handsurgery.org/abstracts/2014/P97.cgi
3 Jann, D., Torbojorn, V., Geisen, T., Muder, D. Interosseous-lumbrical adhesions – a rare condition? A series of five cases. (2021, Dec.) Journal of Plastic Surgery and Hand Surgery. 55(6): 368-372. doi: 0.1080/2000656X.2021.1898972.
4 Muder, D., Torbjorn, V. (2014 Sept 9) Interosseous-lumbrical adhesions secondary to an infection: a case report. Journal of Medical Case Reports. doi: 10.1186/1752-1947-8-301
5 Tan, V., Rothenfluh D.A., Beredjiklian, P.K., Potter, H.G., Weiland, A.J. (2002, July 01). Interosseous-lumbrical adhesions of the hand: Contribution of magnetic resonance imaging to diagnosis and treatment planning. The Journal of Hand Surgery, 27(4). doi: 10.1053/jhsu.2002.33704

Leave a comment